Anaphylaxis Drill Checklist and Anaphylaxis Drill Scenarios
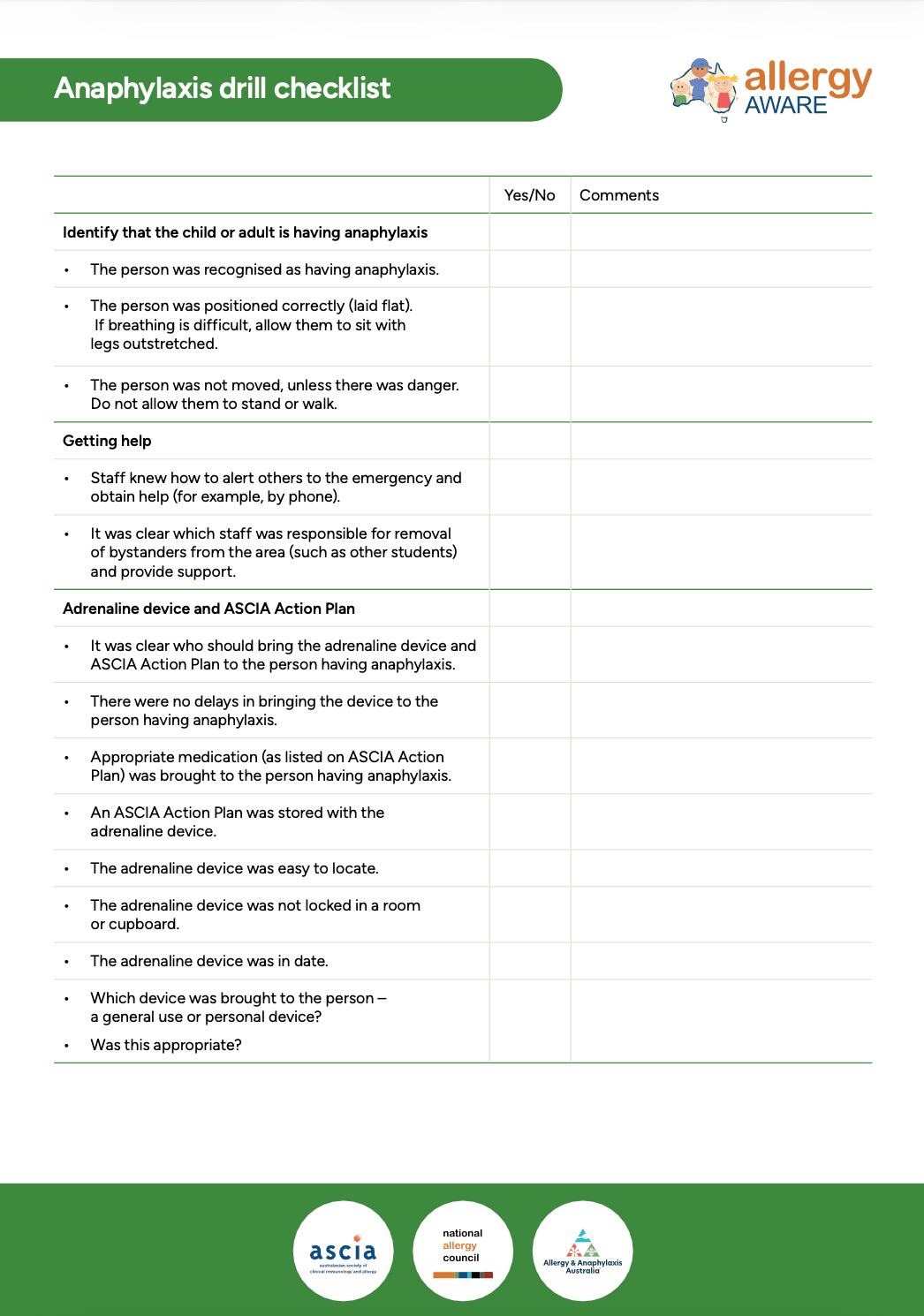
Identify that the child or adult is having anaphylaxis
The person was recognised as having anaphylaxis.
The person was positioned correctly (laid flat). If breathing is difficult, allow them to sit with legs outstretched.
The person was not moved, unless there was danger. Do not allow them to stand or walk.
Getting help
Staff knew how to alert others to the emergency and obtain help (for example, by phone).
It was clear which staff was responsible for removal of bystanders from the area (such as other students) and provide support.
Adrenaline device and ASCIA Action Plan
It was clear who should bring the adrenaline device and ASCIA Action Plan to the person having anaphylaxis.
There were no delays in bringing the device to the person having anaphylaxis.
Appropriate medication (as listed on ASCIA Action Plan) was brought to the person having anaphylaxis.
An ASCIA Action Plan was stored with the adrenaline device.
The adrenaline device was easy to locate.
The adrenaline device was not locked in a room or cupboard.
The adrenaline device was in date.
Which device was brought to the person – a general use or personal device?
ASCIA Action plan
Staff correctly followed instructions on the ASCIA Action Plan according to signs.
Administering the adrenaline device*
Staff followed the steps on the ASCIA Action Plan to correctly administer the device.
Note: The person having anaphylaxis may prefer to administer the device themselves with staff supervision.
The time of administration was recorded.
Calling emergency services
The school has a policy about calling emergency services, communicated to all staff.
It was clear which staff member was responsible for simulating a call to emergency services.
NOTE: A team member could act as the emergency call line and take a simulated call.
The staff member had enough information about the incident to make the call.
Staff member knew school address and had information about where the ambulance should enter.
A staff member was assigned to meet the ambulance staff, and to ensure clear access to the premises.
It was clear which staff member was responsible for communicating details about the incident to ambulance staff.
Staff are aware of school policy regarding accompanying a student in an ambulance.
Monitor the person having anaphylaxis
The ASCIA Action Plan continued to be followed to check for signs of anaphylaxis.
The person was kept in an appropriate position even when they appeared to be recovering.
Staff knew when to administer an additional adrenaline device.
There was a plan in place for getting the additional device. Was it a general use device?
Notify emergency contact
It was clear which staff member was responsible for contacting the child or adult’s emergency contact.
The emergency contact was notified in a timely manner.
Note taking
It was clear which staff member was responsible for recording details of the incident. This includes possible trigger, symptoms, the time adrenaline device given and all actions taken.
Reporting the incident
It was clear which staff member was responsible for completing the report to the appropriate leadership and/or authority.
Debrief and follow up
What went well?
What could have been improved?
Did anything unexpected happen?
Anaphylaxis drill scenarios
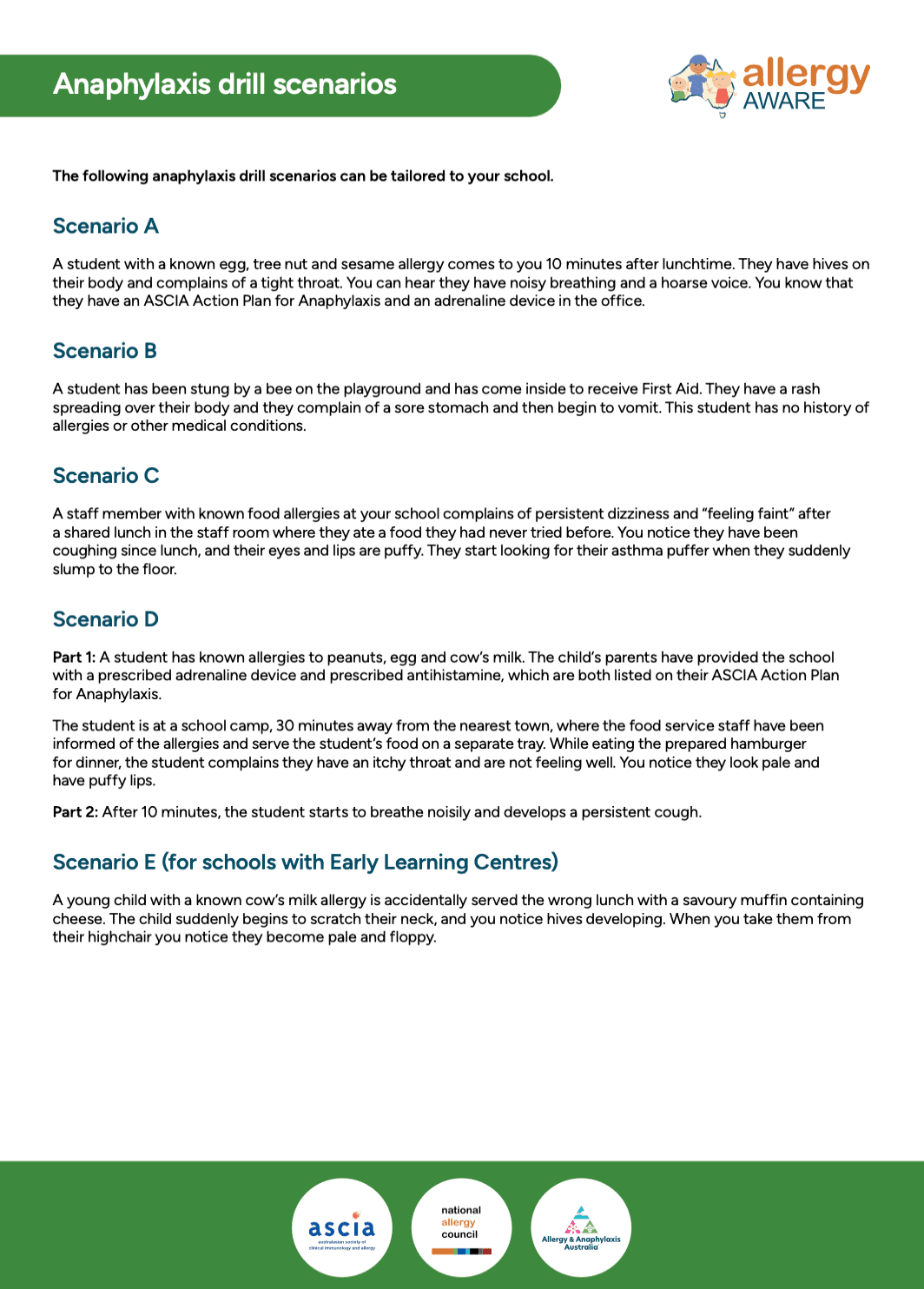
The following anaphylaxis drill scenarios can be tailored to your school.
Consider varying the timing of your drill – running drills before or after school, or during recess or lunch breaks may help identify different issues.
Scenario A
A student with a known egg, tree nut and sesame allergy comes to you 10 minutes after lunchtime. They have hives on their body and complains of a tight throat. You can hear they have noisy breathing and a hoarse voice. You know that they have an ASCIA Action Plan for Anaphylaxis and an adrenaline device in the office.
Scenario B
A child has been stung by a bee on the playground and has come inside to receive First Aid. They have a rash spreading over their body and they complain of a sore stomach and then begin to vomit. This child has no history of allergies or other medical conditions.
Scenario C
A staff member with known food allergies at your school complains of persistent dizziness and “feeling faint” after a shared lunch in the staff room where they ate a food they had never tried before. You notice they have been coughing since lunch, and their eyes and lips are puffy. They start looking for their asthma puffer when they suddenly slump to the floor.
Scenario D
Part 1: A student has known allergies to peanuts, egg and cow’s milk. The child’s parents have provided the school with a prescribed adrenaline device and prescribed antihistamine, which are both listed on their ASCIA Action Plan for Anaphylaxis.
The child is at a school camp, 30 minutes away from the nearest town, where the food service staff have been informed of the allergies and serve the child’s food on a separate tray. While eating the prepared hamburger for dinner, the child complains they have an itchy throat and are not feeling well. You notice they look pale and have puffy lips.
Part 2: After 10 minutes, the student starts to breathe noisily and develops a persistent cough.
Scenario E (for schools with ELC)
A young child with a known cow’s milk allergy is accidentally served the wrong lunch with a savoury muffin containing cheese. The child suddenly begins to scratch their neck, and you notice hives developing. When you take them from their highchair you notice they become pale and floppy.
Content created May 2026.